
Author(s): Avijit Banerjee, Zain Hameed, M. Ali Chohan, Kish Patel, Jin J. Vaghela, Fahad Sheikh, Nick Barker, Pritesh Shah & Divyash Patel
Journal reference: Banerjee, ., Hameed, Z., Chohan, M. et al. Minimum intervention oral care – incentivising preventive management of high-needs/high caries-risk patients using phased courses of treatment. Br Dent J 236, 379–382 (2024).https://doi.org/10.1038/s41415-024-7132-2
Aim
To explore how Minimum Intervention Oral Care (MIOC), supported by phased courses of treatment (CoT), can incentivise preventive management for patients with high treatment needs or high caries risk, whilst also educating clinicians in delivering this type of care.
Background
Traditionally, dental care has focused on restorative treatments such as fillings and crowns once disease has progressed. However, this approach often fails to address the underlying causes of caries and can lead to a repeated cycle of restoration and further tooth damage.
In recent years, dentistry has increasingly focused on preventive and minimally invasive care, hence the development of MIOC to promote early caries detection, disease prevention, and preservation of natural tooth structure. MIOC emphasises longitudinal risk and susceptibility assessments, alongside stabilisation of the oral environment before considering more complex restorative interventions.
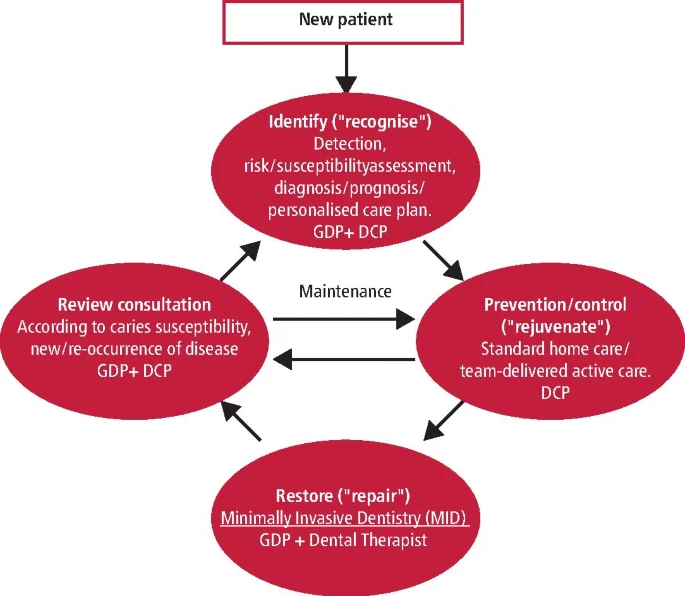
Fig 1. The MIOC approach depicting the four interlinking clinical domains of care: disease identification/ patient assessment, disease control, minimally invasive operative interventions and review. The arrows indicate the direction of patient flow through this cycle.
Methods
The article outlines how MIOC can be implemented through Personalised Care Pathways (PCPs) delivered across multiple CoT within NHS primary care dentistry. This approach recognises that traditional single-course treatment models may not adequately support the long-term management of patients with high caries risk or complex needs. A staged PCP prioritises disease stabilisation and prevention, followed by definitive restorative interventions, whilst allowing care to be tailored to individual patient needs.
The proposed phased model begins with CoT 1, which involves a comprehensive oral health assessment, including diagnosis, prognosis, and initial caries risk/susceptibility assessment (CRSA). A prevention-focused PCP is then developed to stabilise disease. Interventions may include urgent pain relief, temporary restorations, extractions of teeth with poor prognosis, therapeutic sealants, and preventive measures such as oral hygiene instruction, dietary advice, and fluoride application.
Patients then enter CoT 2, which involves reassessment and active surveillance in accordance with NICE and DBOH guidelines. Progression depends on improved disease control and reduced caries risk, after which definitive restorations may be provided.
Patients demonstrating sustained improvement may proceed to CoT 3, where more complex treatments, including indirect restorations or surgical procedures, may be considered if clinically indicated.
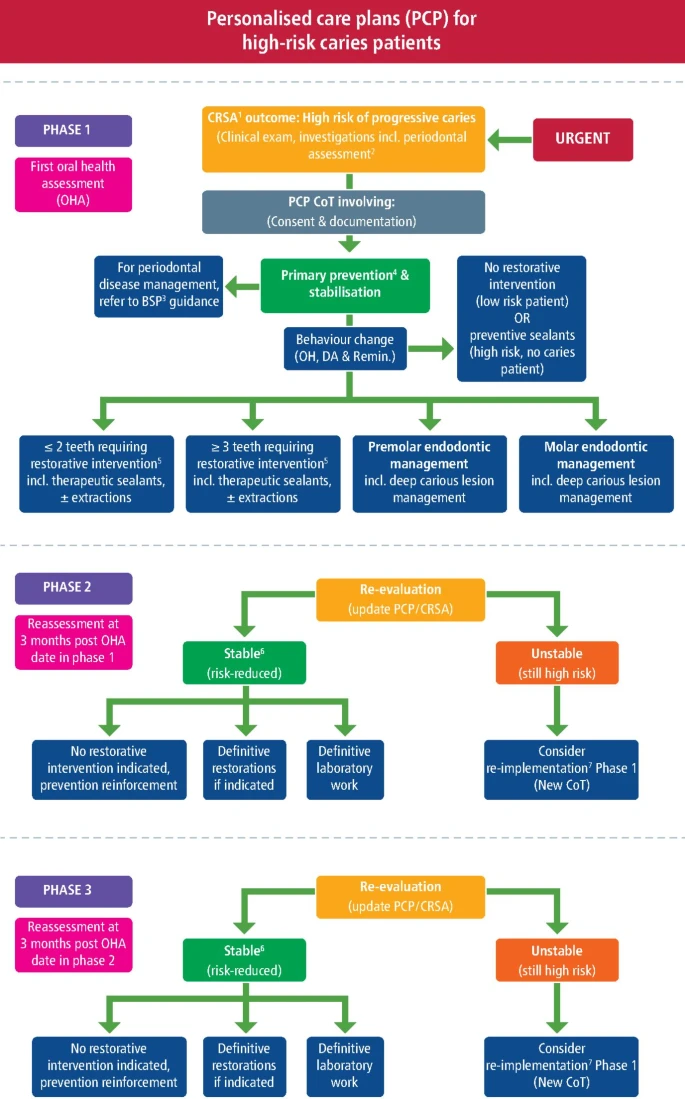
Fig 2. The PCP flowchart for managing high-risk/ needs caries patients, depicting the phased CoT.
Results
The implementation of PCPs through phased CoT encourages a stronger focus on prevention, disease stabilisation, and long-term risk reduction in high caries risk patients. By prioritising early management and behavioural change, clinicians can stabilise the oral environment before undertaking more complex restorative interventions.
Longitudinal caries risk assessments allow clinicians to monitor patient progress and tailor treatment accordingly, helping patients move from high-risk to more stable oral health. As preventative behaviours become established, the likelihood of developing new carious lesions decreases, potentially reducing the need for repeated restorative procedures.
The model also highlights a multidisciplinary dental team approach, enabling shared responsibility for delivering a unified MIOC message – improving efficiency, access to treatment, and patient outcomes.
Conclusion
This paper demonstrates that integrating PCPs and phased CoT within the MIOC framework provides a structured, team-based approach for managing patients with high caries risk. By prioritising disease control, prevention, and risk assessment before restorative care, this approach aims to stabilise oral health, promote long-term disease management and improve patient outcomes.
Research Summary Written By: Nawaira Suhail, University of Manchester – BDS 3