
Geduk, N., Ozdemir, M., Erbas Unverdi, G., Ballikaya, E., & Cehreli, Z. C. (2023). Clinical and radiographic performance of preformed zirconia crowns and stainless-steel crowns in permanent first molars: 18-month results of a prospective, randomized trial. BMC oral health, 23(1), 828. https://doi.org/10.1186/s12903-023-03501-1
Background
First permanent molars (FPM) commonly become carious in children with high caries risk and can often be affected by molar-incisor hypomineralisation (MIH). This means that these teeth are often at risk of multisurface carious lesions and post-eruptive breakdown. FPM with poor prognosis is defined as those with moderate to severe MIH, advanced or unrestorable caries, pulpitits with reversible or irreversible symptoms, radiographically evident pulpal involvement or periradicual pathology. The recommended treatment for poor prognosis FPMs is pulp capping or pulpotomy/ pulpectomy followed by stainless steel crowns or zirconia crowns. The aim of this study was “to investigate the clinical success of compromised permanent molars in children restored with prefabricated metal crowns or zirconia crowns, and the effect of these crowns on periodontal health”.
Methods
A randomised controlled trial was used with a split-mouth design. Participants were recruited from August 2019-January 2021 from Paediatric Dentistry Department after attending for routine dental treatment.
Inclusion criteria: 6-13 years old, healthy, at least two fully-erupted permanent first molars with extensive tissue loss due to multiple (at least 3) carious surfaces with or without MIH. The FPMs cannot effectively be restored with a direct restoration.
Exclusion criteria:
- Non-compliant patients (Frankl Grade 1 and 2 patients)
- Partially-erupted permanent first molars, or fully-erupted ones without an opposing tooth.
- FPM have root canal treatment or deep dentin caries with the risk of iatrogenic pulp exposure.
- Patients with nickel allergy, bruxism and/or deep bite.
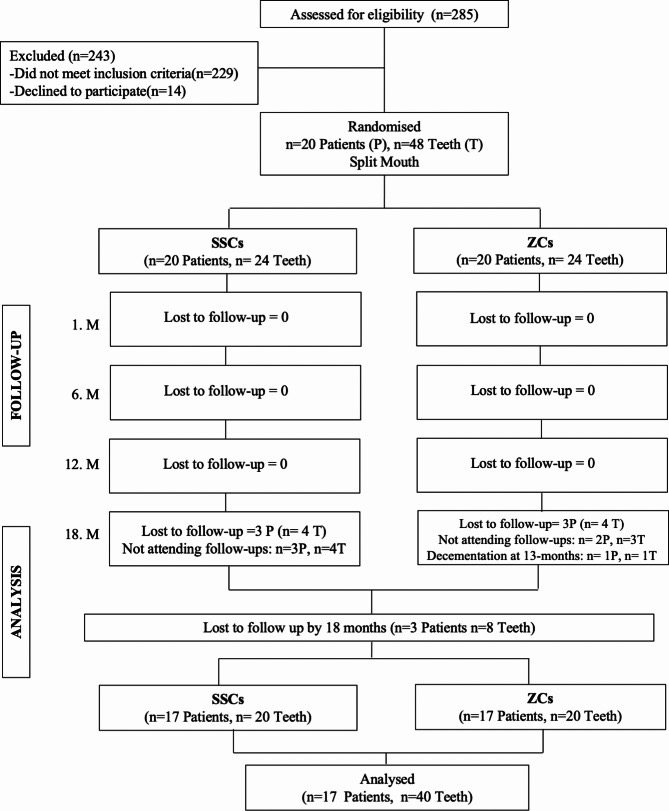
Fig 1: A flow chart showing the participant recruitment process.
A total of 48 FPMs with extensive tissue loss were included in the study and at least two affected FPMs from the same child were randomly assigned to the groups: Group 1 stainless steel crown and Group 2 zirconia crown.
An eperienced, calibrated paediatric dentist performed all treatments. Stainless steel crowns were placed following a conventional technique (with crown preparation and crimped margins and cemented with glass ionomer). The zirconia crowns were placed following preparation and were cemented with light-cured resin-modified glass ionomer.
Clinical assessment was carried out at 1, 6, 12 and 18 months and included evaluation of oral hygiene, gingival health, plaque accumulation, retention, marginal extension of the crown, marginal adaption, periapical health and wear on the oposing tooth. Intra-oral images were taken at baseline and at the follow-ups. Radiographic assessment was performed at 6 and 12 months. The zirconia crowns were also assessed for discolouration and chipping/ fracture.
Blinding was not possible due to the appearance and application procedures of the crowns.
Results
A total of 40 FPM were followed-up to the full 18-months. The mean age was 8 ± 2.49 years and 53% were girls and 47% were boys. The inter-examiner reliability for gingival health determination was 0.87 and the intra-examiner reliability was 0.88 and 0.87. None of the crowns had periapical pathology, discolouration or wear on opposing teeth. The cumulative survival rates at 18 months was 100% for stainless steel crowns and 95.2% for zirconia crowns. There was no significant difference between the median simplified oral health index at baseline and follow-up. For plaque index, the scores for stainless steel crowns were similar at follow-up however the scores for zirconia crowns were significantly lower at follow-up compared to baseline (p<0.001) and these were significantly lower than the scores of stainless steel crowns at all recall periods (p<0.001).
Conclusion
It is recommended that first permanent molars in paediatric patients with multi-surface caries or MIH are restored with stainless steel crowns or zirconia crowns. For the 18 month period of this study, the stainless steel crowns had a higher survival rate compared to the zirconia crowns as one zirconia crown decemented at 12 months. Gingival index and plaque index scores were significantly lower for zirconia crowns compared to baseline and stainless steel crowns.
Research Summary Written By: Ishmyne Bhamra, University of Manchester – BDS 5