
Endodontic treatment is one of the more challenging and time-consuming treatments we provide as dentists. As a student its not something you get to do every day, so remembering the steps, and the right time to take a radiograph can get quite tricky!
Keep reading to get a brief outline of how to manage that daunting root canal treatment you’ve been dreading to start…
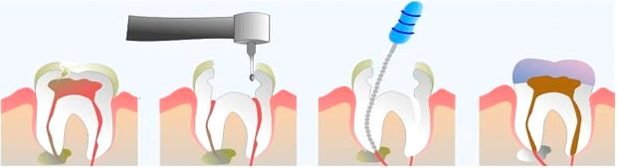
With root canal treatment, the main objectives are to:
- Access
- Clean and Shape
- Fill and Seal
You want to make sure you have a pre-op x-ray to estimate the length of the canal – estimate the length by holding a file against the x-ray (if not digital) or measure using the ruler on centricity. Make a note of the estimated length in your notes, of each canal, and note the coronal reference point you used.
- Finding the canals is arguably the most tricky part of endodontic treatment. If you read textbooks and papers, they recommend a different shaped access for different teeth, however in reality, the tooth you are treating is already so broken down/restored, creating your access isn’t that simple. It is not essential to have a rubber dam on at this point (some may prefer not to use one to avoid drilling the wrong tooth). Once you’ve dropped into the pulp and widened your access, it can help to use an ultrasonic to remove debris to help you see clearer. Once you’ve got your canals, Gates Glidden can be used in a ‘crown down’ manner to widen the orifices very slightly (remember to activate the GG on your outward stroke from the canal, you shouldn’t press the pedal when you’re in the canal or it’ll fracture)
- Establishing the working length is the next step. Go into each canal with a size 10 or 15 file at your estimated working length which you should have from your initial radiograph. Confirm this with either a diagnostic radiograph, or an electronic apex locator – we can alter the working length at this stage depending on what result we get from the apex locator/diagnostic x-ray, and note down the definitive value for each canal (plus the reproducible reference stop you used). It’s worth noting that apex locators can also tell you if there’s a perforation.
- Now you’re ready to start preparing your canals to your definitive working length (WL). Your Master Apical File (MAF) should go down to your WL – this file should be at least two sizes larger than you Initial Apical File (IAF), which is the one you used to determine your WL (usually a 10/15). Use the step back technique and clean up the canal, coming higher 1mm at a time, with each bigger file size. Remember to ALWAYS RE-CAPITULATE AND IRRIGATE in between files. Never let the needle catch when irrigating always keep it moving. Ensure you have tug-back at your WL.
- Obturation of the canals is the next step. Once you’re sure you’ve cleaned and shaped your canals, dry them thoroughly with paper-points. You’ll use the lateral condensation technique to obturate, so get a gutta percha point the same size as you MAF. Measure this to your WL and try it in the canal. You can take a dry run xray if you want, to confirm the GP point is at the correct length. When you’re happy, you can dip this in tubliseal and pack it laterally against the wall of the canal. Keeping the canal dry is really important. Get accessory files and place these next to this GP point and pack laterally again. Keep going until you’re happy you’ve filled the canal to avoid any voids.
- Removing excess GP using a hot instrument is next. Ask your nurse to heat the end of the instrument on the Bunsen burner and hand it straight to you making sure you’re ready and in position to swiftly remove the GP. You must be swift but also accurate when removing this, as you don’t want to pull out all the GP you’ve placed – so chop it from the level of the orifice of the canal, and let the instrument do the work slowly, as opposed to you slicing the GP with force. Make sure you’re not too slow as the instrument is hot and you don’t want to harm the patient or yourself.
- Finally you should place a coronal seal using RMGI such as vitrebond or flowable composite.
- FGDP endodontic follow-up guidelines state a post-op radiograph must be taken before the patient leaves the practice after the endodontic treatment is completed, to assess the success of the obturation, and to act as a baseline for assessment of apical pathology or healing. There is still debate as to when to take the follow-up radiograph, but a widely accepted time gap, post treatment is 1 year to assess healing of peri-radicular disease.